
The ideal dental cement should possess several characteristics. It should be non-irritating to the dental tissues, possess a low film thickness, be insoluble in oral fluids, have the ability to close gaps that are present at the margins of restorations, be simple to use, be easy to clean up, possess good adhesion to a variety of dental materials, be identifiable on a radiograph (radiopaque) and provide sustained results over a prolonged period of time.1 While many current cements offer an array of different benefits, many come with substantial limitations or negative characteristics that prohibit them from being classified as the “perfect” dental cement.
Background on Dental Cements
Dental cements can be divided into six primary groups with a seventh additional group that will be discussed in this article:
1) Zinc Phosphate Cement
2) Polycarboxylate Cement
3) Glass Ionomer Luting Cement
4) Polyacid-Modified Composite Cement
5) Resin-Modified Glass Ionomer Cement
6) Resin-Based Cement
7) Bioceramic Luting Cement (Newest Addition to Cement Choices)
Zinc Phosphate Cement
This cement has a long track record in dentistry with well over one century of use. Zinc Phosphate is relatively inexpensive, easy to mix and clean up and is radiopaque. Unfortunately those benefits are overshadowed by several glaring shortcomings that include a very low pH, relatively low bond to tooth structure and solubility in oral fluids. The biggest issue with this cement is the fact that it routinely induces a pulpitis due to its irritating nature. This often results in prolonged sensitivity to temperature changes.2
Polycarboxylate Cement
Polycarboxylate cement has a number of benefits that include that it does not routinely induce a pulpitis and it has relatively strong bonds to tooth structure. The biggest issues with Polycarboxylate cements are that they can be quite difficult to clean up and undergo a relatively fast viscosity change following mixing. This makes them fairly difficult to control and manipulate.2
Glass Ionomer Luting Cement
These cements have many positive characteristics that make them relatively desirable in the dental marketplace. One of the greatest advantages is fluoride release. Glass ionomer cements also possess good adhesion to both enamel and dentin and form relatively strong bonds. These benefits are offset by several substantial limitations that include the fact that glass ionomers can take up water during setting, changing the physical characteristics. Due to their acidic nature, they can also be irritating to pulpal tissues. This may lead to pulpitis following cementation.
Polyacid-Modified Composite Cement
This group has some distinct advantages over other types of cements that include relatively high bond strengths to tooth structure and relatively low solubility in oral fluids. Unfortunately they undergo hygroscopic expansion and lose bond strength over a fairly short period of time.3
Resin-Modified Glass Ionomer Cement
Resin-modified glass ionomer cements have been used in dentistry for several decades and possess several advantages. These cements are simple to mix and clean up, are relatively stable over a long period of time, possess some potential for fluoride release and generally have favorable handling characteristics.4
On the other hand, they are acidic in nature with the potential of inducing a pulpitis and are moisture sensitive due to their hydrophilic nature. These negative properties detract from their potential to be the “perfect” dental cement.
Resin-Based Cement
This fairly large group of cements can be either auto curing or cured exclusively with a dental curing light. They come in a variety of different configurations that include self-etching versions or cements that require the use of a separate adhesive system to maximize results. The adhesive bonds established with the self-etching versions tend to be lower than those established with systems utilizing separate etching and bonding.5 Resin based cements have several major advantages over other groups of cements: high bond strengths to tooth structure, relative insolubility in oral fluids and when used correctly they generally do not irritate pulpal tissue. They are the ideal cement when bonding relatively low strength dental ceramics. However, these cements are also the most technique sensitive of all types of cement. Bond strength can be dramatically affected if proper technique is not utilized or contamination occurs during bonding. Additionally, many of these cements require multiple steps and can be quite difficult to clean up after complete curing. While many resin cements are radiopaque,6 some are not, making them difficult to identify on radiographs.
Bioceramic Luting Cement
This category encompasses the most recent developments in cement technology. Currently, there is only one commercial product available in this class and it is rapidly gaining traction – Ceramir C&B® bioceramic luting cement from Doxa Corporation. The cement is a water-based hybrid composition of calcium aluminate and glass ionomer components. While the mechanism of cement setting is similar to that of conventional GICs, the presence of calcium aluminate provides some very unique properties.7 The balance of the article will discuss the benefits and characteristics of this cement class.
Dental Tissue Compatibility
When parameters like pulpal inflammation, gingival response and cytotoxicity were examined; Ceramir demonstrated little to negligible negative responses from adjacent dental tissues. These reactions are in stark contrast to the known response parameters expected with acid and resin based conventional cements.The characteristic of being non-irritating to tissue makes this cement very suitable for use when interfaces include close proximity to pulpal borders, as well those that encroach on or extend below the gingival margin.8,9 In particular, this is very advantageous when delivering cement retained implant supported restorations. The sequelae related to undetected cement extrusion around implants are well documented. While best practices in removal of extruded cement are always recommended, inevitably there are detection challenges specific to clinical practice. These include subgingivally extended margins, obscured buccal and lingual interfaces on radiographs, etc. In the event that small particles of cement are left behind, the most tissue friendly cement would be the best choice. Figures 1a and 1b show a posterior cement retained implant crown that was just cemented with Ceramir Bioceramic Luting Cement. The radiopacity of the residual cement is clearly evident on the distal aspect of the restoration upon inspection of a verification radiograph. The second radiograph verifies the removal of all residual cement. Figure 2a shows an anterior implant case in progress with a provisional implant borne restoration in place for the upper right lateral incisor. The proposed final restoration back from the lab is presented on the working model (Fig. 2b). Figure 3a shows the verification radiograph of the custom abutment torqued into place and figure 3b shows the clinical image of the zirconia abutment in the process of screw access closure. Figures 4a, 4b and 4c show the three-step process of fabricating a provisional PVS abutment copy, loading of the final crown with Ceramir and delivering the crown to the copied abutment for cement management. This strategy for cement extrusion and clean up extra-orally is one of the predictable methods employed by practitioners to mitigate the incidences of excess cement extrusion. After primary cement clean up, the crown is then transferred to the abutment in place in the mouth with the slightest amount of residual cement easily cleaned prior to complete set. Images 5a and 5b show the final radiographic image and clinical photo of the final crown in place.
FIGURE 1A. Opaque cement is visible post.
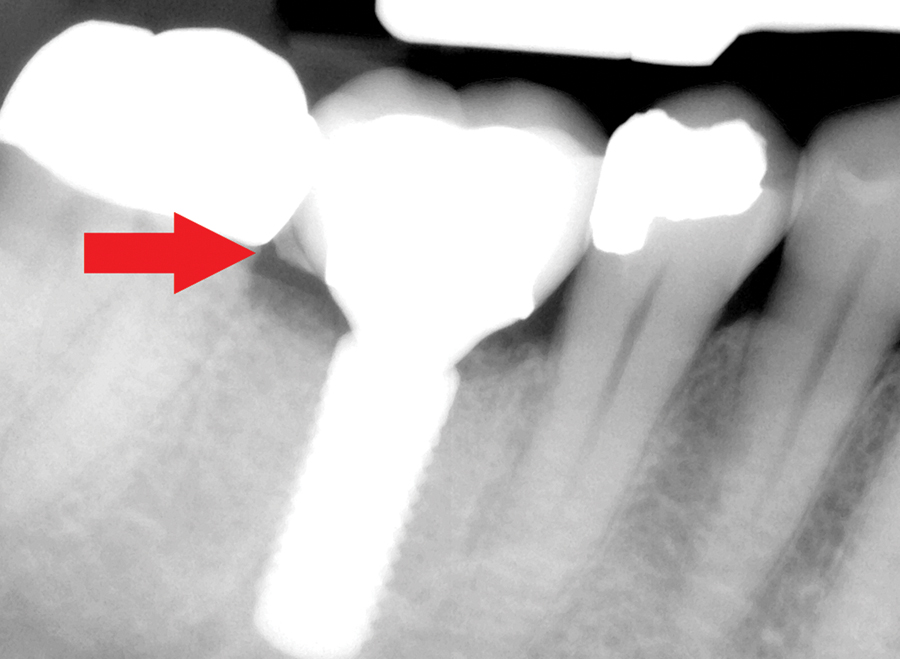
FIGURE 1B. Cement removal verified.
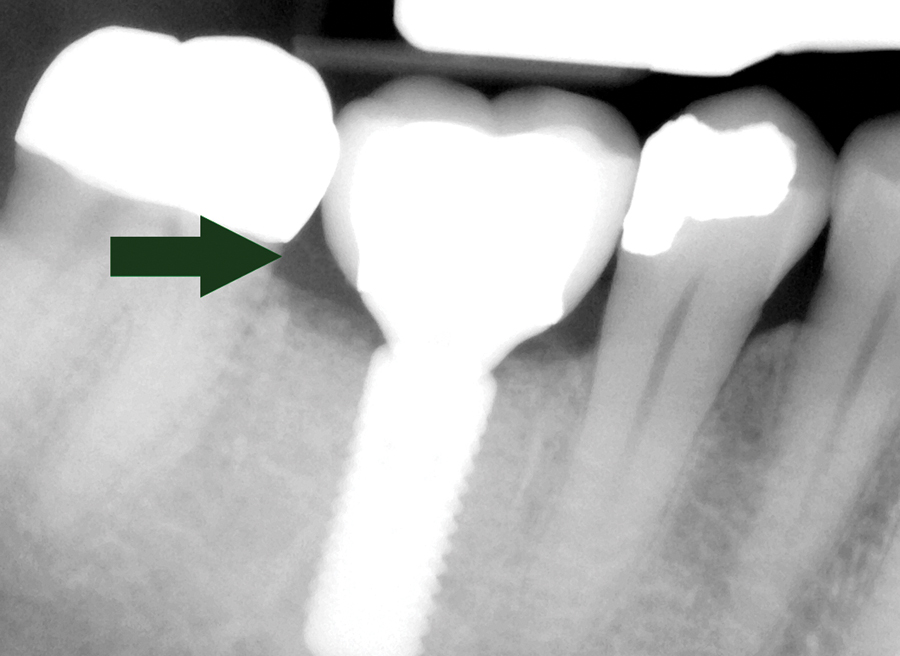
FIGURE 2A. Implant retained provisional crown in place.

FIGURE 2B. Final lithium disilicate crown for tooth 12 displayed on working model.

FIGURE 3A. Verification radiograph of abutment in place.

FIGURE 3B. Occluding screw hole of custom zirconia abutment in position.

FIGURE 4A. Copy abutment fabrication.

FIGURE 4B. Final crown loaded with Ceramir bioactive cement.

FIGURE 4C. Excess cement displacement after seating on copy abutment.

FIGURE 5A. Verification radiograph showing no residual cement.
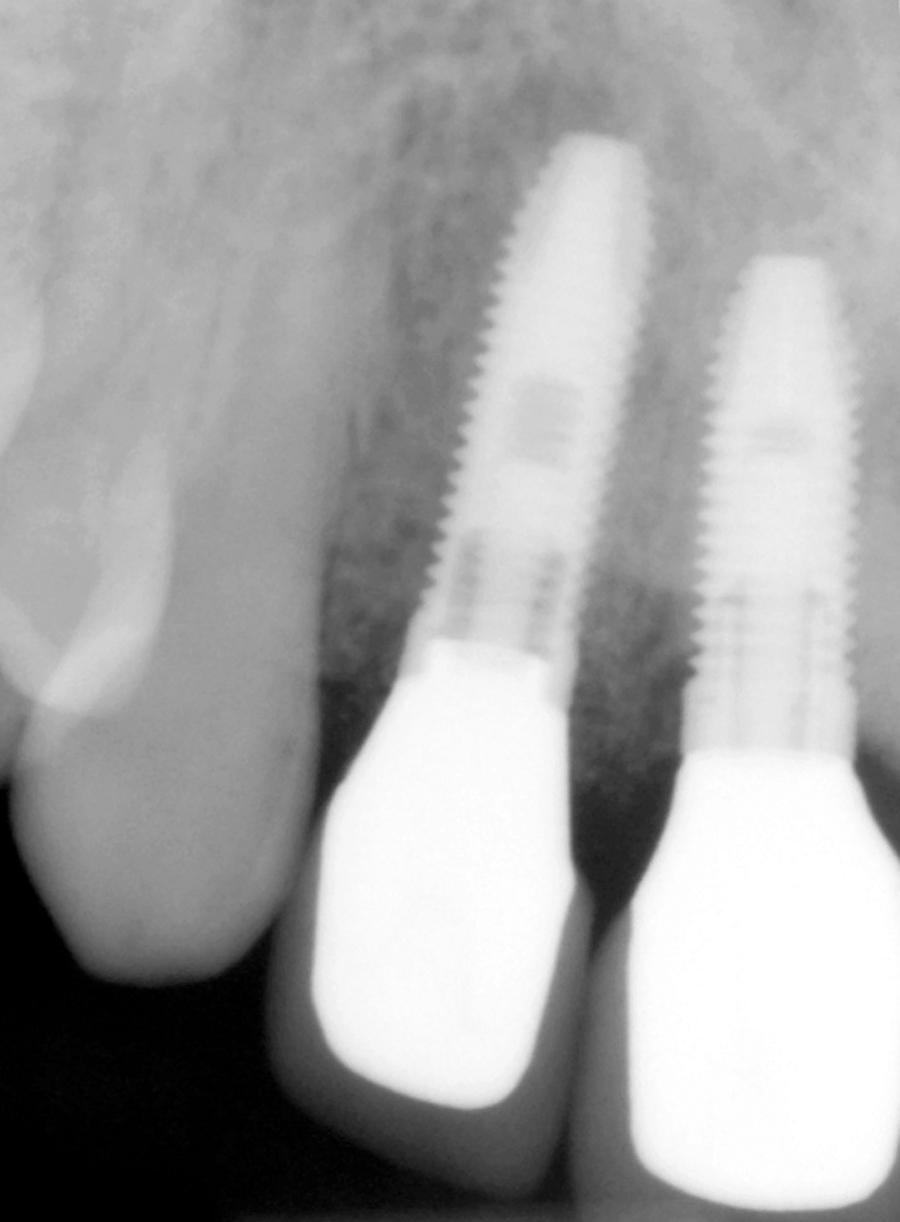
FIGURE 5B. Clinical photo of final crown.

Low Film Thickness
The film thickness of Ceramir has been measured at around 16 microns. This facilitates the complete seating of all restorations without difficulty, including those with more parallel retention profiles. Flow characteristics not only allow for cement displacement upon reasonable seating pressure but also support easy wetting of intaglio surfaces when the cement is loaded. Fortunately, the fluid behavior of Ceramir does not prohibit the practitioner from inverting a loaded restoration. This relative viscosity prevents cement from dripping out of a restoration during handling.
Handling and Use
Ceramir is delivered through activation, trituration and extrusion instrumentation similar to that of conventional GIC capsules (Fig. 6). Doxa is in the process of updating the mechanics of this delivery with the goal of also providing an auto-mix formulation for convenience. Another attractive characteristic of this bioceramic cement is the working and setting time. After activation and trituration, a slightly longer working time is afforded to the practitioner when compared to other luting cements. This greatly reduces the possibility of premature set or rushed delivery. As soon as the restoration is subjected to the warmth of the oral cavity, the gel time is accelerated and the ideal cement removal window is not delayed. Clean up is accomplished very easily compared to resin based cements where cement removal can prove challenging at times.
FIGURE 6. Delivery instrumentation.

Mechanical and Physical Characteristics
Bioceramic cements have indications for use across all metal and ceramo-metal indirect restorations, metallic posts, inlays and onlays, monolithic zirconia restorations, zirconia and alumina framework based ceramics and lithium disilicate restorations. Because of this wide spectrum of applications, it is noteworthy that the retentive quality is measured to be on par with or better than conventional alternatives. Tables 1, 2 and 3 show relative retention and adhesion values across several substrates including tooth structure when compared to other conventional cement options.10,11 Ceramir reports a 24-hour compressive strength of 160 MPa with progressive escalation to 210 MPa after 90 days. Modulus of elasticity is reported at 4.7 GPa and radiopacity is reported at 1.5 mmAl.
TABLE 1. Comparative retention values of a variety of cements.
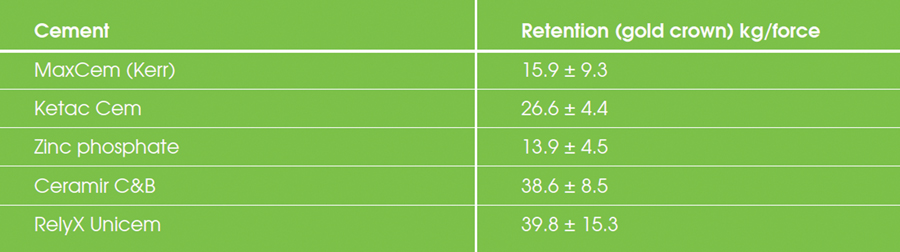
TABLE 2. Retention of zirconia crown comparison.

TABLE 3. Comparative shear bond strength measurements across a variety of substrates.

Bioactivity and Behavior
Considering all of the benefits listed to this point related to “ideal” bioceramic cements, perhaps the most critical factor is in fact the possibility of bioactivity and any derived benefits. The first of these critical factors is pH. Reduced pH is linked to both pulpal sensitivity as well as bacterial related cariogenic activity. Ceramir reaches a basic pH of approximately 8.5 within a few hours of placement, which is maintained throughout service.7 This basic pH can create a cariostatic environment for the life of the restoration.
Another critical factor is apatite formation and remineralization. Initial fluoride release in Ceramir is comparable to that of GICs and similarly decreases over time. However, incorporation of Calcium Aluminate and the abundance of Ca 2+ ions allows for continued apatite formation and bioactivity. In fact, a recent laboratory study suggests the possibility of marginal interface and marginal gap closure (i.e. restoration margins) via surface apatite forming bioactive cements. This phenomenon was not evident with conventional acid based resin cements.12 In essence, the potential ability of a bioceramic cement to shrink or occlude the restorative marginal gap is now supported and should have a significant impact on the conventional approach to restorative delivery.
Conclusion
Dental cements have evolved significantly over the years. Several reliable cement classes have overcome the challenges of retention quite predictably. Practitioners seem to choose cements based on a number of factors, which typically include retention requirements (based on preparation design and restorative material being cemented), ease of use and esthetic considerations.
An evolving consideration is that of “bio-activity and bio-compatibility”. This trend is mirrored and further developed in the direct restorative arena. It is the opinion of the authors that this same trend will continue to develop in the category of luting cements and should be a consideration when cements are selected. This will improve clinical outcomes, restorative longevity and patient health. OH
Foroud Hakim, DDS, MBA, BS; Assistant Professor and Vice-Chair, Department of Integrated Reconstructive Dental Sciences, University of the Pacific, School of Dentistry.
Marc Geissberger, DDS, MA, BS; Professor and Chair, Department of Integrated Reconstructive Dental Sciences, University of the Pacific, School of Dentistry.
Oral Health welcomes this original article.
References:
1. Michael S. Jacobs, D.D.S., M.S., A. Stewart Windeler, D.D.S., M.Sc., Ph.D. An investigation of dental luting cement solubility as a function of the marginal gap. Journal of Pros Dent. March 1991:Volume 65, Issue 3, Pages 436–442.
2. Komal Ladha, Mahesh Verma. Conventional and Contemporary Luting Cements: An Overview. J Indian Prosthodont Soc. 2010 Jun; 10(2): 79–88.
3. M.A. Cattani-Lorentea, V. Dupuisb, F. Moyac, J. Payanc, J.-M. Meyer Comparative study of the physical properties of a polyacid-modified composite resin and a resin-modified glass ionomer cement. Dental Materials. 15 (1999) 21–32.
4. Sidhu SK, Watson TF. Resin-modified glass ionomer materials. A status report for the American Journal of Dentistry. American Journal of Dentistry. 1995: 8(1):59-67.
5. Sahar E. Abo-Hamar, Karl-Anton Hiller, Heike Jung, Marianne Federlin, Karl-Heinz Friedl, Gottfried Schmalz. Bond strength of a new universal self-adhesive resin luting cement to dentin and enamel. Clinical Oral Investigations. September 2005, Volume 9, Issue 3, pp 161-167.
6. Pekkan, Mutlu Özcan. Radiopacity of different resin-based and conventional luting cements compared to human and bovine teeth. Dental Materials. Vol. 31 (2012) No. 1 P 68-75.
7. J Lööf, F Svahn, T Jarmar, H Engqvist, C H Pameijer, Dental Materials, Vol 24 (5), 653-659 (2008).
8. L, Saksi M, Hermansson L, Pameijer CH. A five-year retrospective clinical study of calcium-aluminate in retrograde endodontics. J Dent Res 2008 Abstr#1333, Vol 88 Special Issue B.
9. Jefferies S, Pameijer CH, Appleby D, Boston D. One Month and Six Month Clinical Performance of Xera-Cem, J Dent Res., 2009; 88(A):3146.
10. CH, Jefferies SR, Lööf J, Hermansson L, A Comparative Crown Retention Test Using Xera-Cem J Dent Res., 2008;87(B):3099.
11. Jefferies SR, Lööf J, Pameijer CH, Boston D, Galbraith C,Hermansson L., Physical Properties of Xera-Cem, J Dent Res. 2008; 87(B):3100.
12. Jefferies S, Fuller A, Boston D, Preliminary Evidence That Bioactive Cements Occlude Artificial Margin Gaps JERD, Mar. 2015











