
Abstract
Understanding the hard and soft tissue changes of post-extraction sockets and the condition of the anatomy of the future implant site is essential for clinicians in deciding when and where future implants should be placed. This report provides a simplified decision making protocol that will help guide clinicians on the timing of implant placement.
Timing for Implant Placement after Single Tooth Extraction
Dental implants have been reported to have long-term success in the rehabilitation of completely, or partially edentulous patients. The focus for implant therapy has since shifted from osseointegration to esthetic restoration that is stable over time.1,2 Various factors need to be evaluated during preoperative planning,3 and the timing of implant placement post-extraction is considered an important factor which influences the esthetic outcome.4
Traditionally, compromised teeth were removed and the resultant extraction sockets were left to heal for four to six months before dental implants were placed.5 However, marked alterations occur in the edentulous site following extraction, not only in the buccal–lingual/palatal dimension (about 50 percent), but the height of the buccal bone crest also decreases.6,7 Improved implant hardware coupled with patient demand has shifted research focus towards shortened post-extraction healing time or immediate implant placement following extraction.8 It has been suggested that the placement of an implant in the fresh extraction socket may counteract alveolar ridge contraction following tooth removal,9,10 However, this hypothesis was not validated in recent humans and animals studies (Fig 1).11-13
FIGURE 1.

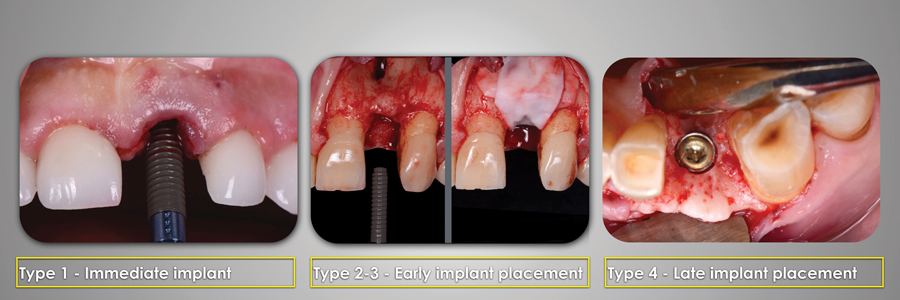
Four different implant placement protocols have been defined based on the bone remodeling process:
Immediate or type 1, when the implants are placed in the same surgical intervention as the dental extraction
Type 2 or early implant placement with soft tissue healing, wwhen implants are placed in the early stages of healing (from four to eight weeks)
Type 3 or early implant placement with partial bone healing (12 weeks to 16 weeks)
Type 4 late implant placement, when the extraction socket is fully healed (after 16 weeks) (Fig 2).14
FIGURE 2.
The objective of this article is to describe the implant placement protocols, their indications, advantages and risk factors.
RELATED VIDEO: Using Screw Retained Implant Restorations
Immediate Implant Placement: Type 1
Although the first clinical procedures for the placement of implants immediately following tooth removal were described long ago, it is only recently that the details of such clinical approaches have been studied in greater detail.14 The advantages of immediate implant placement are: reduction of treatment time, fewer surgical interventions and a decrease in surgical trauma to the soft tissues at the implant site.15 However, unpredictable gingival recession and crestal bone resorption have been associated with immediate implant placement in the esthetic zone.16 Various key factors have been described to minimize the complications.
Facial Bone Integrity
It has been identified that pre-existing defects of the facial bone are associated with recession of the facial mucosa on immediate implants.17 It is therefore recommended that the tooth to be replaced be extracted atraumatically to avoid damaging the extraction socket. Furthermore, the integrity of an intact buccal plate should be located no more than 4mm apically from the free gingival margin.18
Facial Bone Thickness
It has been determined that a minimal width of 2mm of buccal bony wall is a prerequisite to maintain the vertical dimension of the alveolar crest over time.19,20 However, according to a recent study, 87 percent of the buccal bony walls on anterior sites have a thickness of 1 mm or less21 and are therefore prone to resorb. In order to counteract this situation, lingualized placement of implants resulting in a buccal horizontal gap between the socket and the implant is recommended.22
Horizontal Gap
When immediate implants are placed, peri-implant voids are frequently present due to a gap between the alveolar socket and the implant.23 It is recommended that the implant be placed 2mm lingual and 1mm apical to the buccal plate and the gap filled with xenogenic grafting material of a low resorption rate, in order to compensate for the expected bone resorption process.24-26 The use of a provisional restoration or a customized healing abutment over the implant for the sealing of the socket has been recommended. This is to maintain the blood clot and bone graft material in the healing phase of treatment.27
Primary Stability
An adequate primary stability is recommended to ensure a successful immediate implant with or without an immediate provisional restoration.17 This can be achieved by engaging the implant to the palatal and apical bony region approximately 3 to 4mm beyond the apex of the socket, where cancellous bone predominates.28 A recent study demonstrated that in 81 percent of cases, roots of anterior teeth are positioned against the cortical plate, which results in a considerable amount of bone in the palatal area.29 This ideal clinical scenario allows placement of a properly engaged immediate implant. It is therefore important to evaluate the sagittal root position of the tooth to be extracted in a CBCT prior to implant placement.
Thickness of Soft Tissues
The peri-implant biotype is categorized as thin, if the outline of an underlying periodontal probe can be seen though the gingiva; and thick, if the probe cannot be seen.30 Recent studies have shown that immediate implant placement with immediately placed provisional restorations at sites with thin biotypes had significantly more recession than thick biotype sites after one-year (0.75 vs 0.25mm respectively).31 It has been reported that the presence of a thin biotype, smoking, presence of a thin buccal plate and facially positioned implants are the main risk factors for mucosal recession in immediately placed implants. A recent article has described the use of connective tissue grafts to transform a thin biotype into a thick biotype when placing immediate implants;32 the cases where this technique was used experienced less facial gingival level changes.33
Early Implant Placement: Type 2 and Type 3
In cases where the alveolar socket is compromised and potential risk factors for placing immediate implants are present, the early implant placement protocol has been proposed. The main objectives of this protocol are: to ensure the lack of pathology when placing the implant, to optimize the availability of soft tissues for primary healing and to achieve a successful contour augmentation of the buccal aspect of the implant.
The Type 2 protocol is characterized by extraction of the tooth without flap elevation, debridement of the socket, followed by a four to eight week soft tissue development over the extraction socket, implant placement with simultaneous guided bone regeneration using a bio-absorbable collagen membrane with autogenous bone chips combined with a slow resorbing bone substitute and tension free primary closure (Fig 3). The waiting time for the soft tissues to mature over the area where the implant is placed in combination with guided bone regeneration will provide protection for the biomaterials against bacteria from the oral cavity and reduce the risk of postsurgical complications.34,35
FIGURE 3.

between four to eight weeks post extraction.
The Type 3 implant placement is another type of early implant placement protocol characterized by a 12 to 16 week delay of the treatment after tooth extraction; this provides substantial bone fill of the socket that facilitates implant placement and mature soft tissues that facilitate flap management. The early implant placement protocols have been proven to have a low risk for mucosal recession, successful esthetic outcomes and good long-term stability of the established facial bone wall.35,36
Late Implant Placement: Type 4
In the late 80s, a post-extraction healing period of four to 12 months prior to implant placement was considered the standard of care because a fully healed ridge ensures implant insertion in a stable ridge dimension. In cases where pathology has completely affected the socket integrity, primary stability of an implant cannot be achieved, or limiting anatomical structures are difficult to avoid, waiting for complete healing of the site may still be the treatment of choice. However, in many of these cases the bone availability for an implant to be placed in an optimal 3D implant position may not always be ideal due to the resorptive changes after tooth extraction; therefore regenerative procedures may be needed.37
Conclusion
The soft and hard tissue changes following tooth extraction are in close relationship to the timing of the implant placement. In spite of similar success rates reported for immediate, early and delayed placement, it is very important to understand the risk factors related to each procedure, to have careful case selection and to closely follow the surgical and prosthetic protocols.OH
After graduating from the Universidad San Martin de Porres dental school in Peru, Dr. Daniel Ochoa pursued an advanced program in Oral Rehabilitation at D.A.T.O Institute, Buenos Aires, Argentina. He then undertook a thorough program of continuing education courses on esthetics and prosthodontics worldwide and studied at the Advanced Program in Implant Dentistry at NYU College of Dentistry. Dr. Ochoa is a Diplomate of the ICOI, Fellow of the ICOI and IADFE, member of the AACD, ASDA, ITI, AO and DSD Masters group, He has lectured nationally and internationally and is currently dedicated to his private practice and is Co-director of the Infinity–Institute for Advanced Dental Learning in Lima, Peru.
Dr. Takanori Suzuki received his DDS degree at Nippon Dental University College of Dentistry in 2000. He completed his PhD in Operative Dentistry in 2004 at the same university. He then studied at the Advanced Program in Implant Dentistry at NYU College of Dentistry and continued in the Clinical Fellowship Program in Implantology at NYU-College of Dentistry. He is currently Clinical Assistant Professor at NYU-College of Dentistry’s Implant Department, Fellow of the ICOI, Diplomate of the ICOI, and has published numerous articles and lectured internationally.
Oral Health welcomes this original article.
References:
1. Jemt T. 2008–Single implants in the anterior maxilla after 15 years of follow-up: comparison with central implants in the edentulous maxilla. Int J Prosthodont. Sep-Oct;21(5):400-408.
2. Tonetti, M.S., Hammerle, C.H. European Workshop on Periodontology Group C. (2008) Advances in bone augmentation to enable dental implant placement: Consensus Report of the Sixth European Workshop on Periodontology. Journal of Clinical Periodontology 35(Suppl): 168–172.
3. Buser, D., Martin, W. & Belser, U.C. (2004) Optimizing esthetics for implant restorations in the anterior maxilla: anatomic and surgical considerations. The International Journal of Oral & Maxillofacial Implants 19(Suppl): 43–61.
4. Chen, S.T. & Buser, D. (2009) Clinical and esthetic outcomes of implants placed in postextraction sites. The International Journal of Oral & Maxillofacial Implants 24(Suppl): 186–217.
5. Quirynen M, Assche N, Botticelli D, Berglundh T. How does the timing of implant placement to extraction affect outccome? Int H Oral Maxillofac Implants 2007;22(suppl): 203-223
6. Schropp, L., Wenzel, A., Kostopoulos, L. & Karring, T. (2003) Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. The International Journal Periodontics Restorative Dentistry 23: 313–23.
7.
Botticelli D, Persson LG, Lindhe J, Berglundh T. Bone tissue formation adjacent to implants placed in fresh extraction sockets: an experimental study in dogs. Clin Oral Implants Res. 2006 Aug;17(4):351-358.
8. Esposito M, Grusovin M, Polyzos I, Felice P, Worthington H. Timing of implant placement after tooth extract immediate, immediate-delayed or delayed implants? A Cochrane systematic review. Eur J Oral Implantol 2010;3(3):189–205.
9. Denissen H, Kalk W, Veldhuis H, Van Waas M. Anatomic consideration for preventive implantation. Int J Oral Maxillofac Implants. 1993;8(2):191-196.
10. Watzek G, Haider R, Mensdorff-Pouilly N, Haas R. Immediate and delayed implanta- tion for complete restoration of the jaw following extraction of all residual teeth: a retrospective study comparing different types of serial immediate implantation. Int J Oral Maxillofac Implants. 1995 Sep-Oct;10(5):561-567.
11. Botticelli D, Berglundh T, Lindhe J. Hard-tissue alterations following immediate implant placement in extraction sites. J Clin Periodontol. 2004 Oct;31(10):820-828.
12. Araujo M, Sukekava F, Wennstrom J, Lindhe J. Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog. J Clin Periodontol. 2005 Jun;32(6):645-652.
13. Araujo M, Sukekava F, Wennstrom J, Lindhe J. Tissue modeling following implant placement in fresh extraction sockets. Clin Oral Implants Res. 2006 Dec;17(6):615-624.
14. Hämmerle CH, Chen ST, Wilson TG. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int J Oral Maxillofac Implants. 2004;19 Suppl:26-28.
15. Froum SJ, Cho SC, Francisco H, Park YS, Elian N, Tarnow DP. Immediate implant placement and provisionalization–two case reports. Pract Proced Aesthet Dent. 2007 Nov-Dec;19(10):621-628.
16. Kan JY, Rungcharassaeng K, Lozada JL, Zimmerman G. Facial gingival tissue stability following immediate placement and provisionalization of maxillary anterior single implants: a 2- to 8-year follow-up. Int J Oral Maxillofac Implants. 2011 Jan-Feb;26(1):179-187.
17. Kan JY, Rungcharassaeng K, Sclar A, Lozada JL. Effects of the facial osseous defect morphology on gingival dynamics after immediate tooth replacement and guided bone regeneration: 1-year results. J Oral Maxillofac Surg. 2007 Jul;65(7 Suppl 1):13-19.
18. Chu SJ, Salama MA, Salama H, Garber DA, Saito H, Sarnachiaro GO, Tarnow DP. The dual-zone therapeutic concept of managing immediate implant placement and provisional restoration in anterior extraction sockets. Compend Contin Educ Dent. 2012 Jul-Aug;33(7):524-32, 534.
19. Spray, J.R., Black, C.G., Morris, H.F. & Ochi, S. (2000), The influence of bone thickness on facial marginal bone response: stage 1 placement through stage 2 uncovering. Annals of Periodontology 2000 (5): 119–128.
20. Grunder, U., Gracis, S. & Capelli, M. (2005) Influ- ence of the 3-D bone-to-implant relationship on esthetics. Int J Periodontics Restorative Dent. 2005 Apr;25(2):113-119.
21. Huynh-Ba G, Pjetursson BE, Sanz M, Cecchinato D, Ferrus J, Lindhe J, Lang NP. Analysis of the socket bone wall dimensions in the upper maxilla in relation to immediate implant placement. Clin Oral Implants Res 2010: 21: 37–42.
22. Lee E, Gonzalez-Martin O, Fiorellini J. Lingualized Flapless Implant Placement into Fresh Extraction Sockets Preserves Buccal Alveolar Bone: A Cone Beam Computed Tomography Study. Int J Periodontics Restorative Dent 2014;34:61–68.
23. Capelli M, Testori T, Galli F, Zuffetti F, Motroni A, Weinstein R, Del Fabbro M. Implant–Buccal Plate Distance as Diagnostic Parameter: A Prospective Cohort Study on Implant Placement in Fresh Extraction Sockets. J Periodontol. 2013 Dec;84(12):1768-1774.
24. Vignoletti F, Sanz M. Immediate implants at fresh extraction sockets: from myth to reality. Periodontol 2000. 2014 Oct;66(1):132-152.
25. Araujo M, Lindhe J. Bio-Oss Collagen in the buccal gap at immediate implants: a 6-month study in the dog. Clin Oral Implants Res. 2011 Jan;22(1):1-8.
26. Tarnow DP, Chu SJ, Salama MA, Stappert CF, Salama H, Garber DA, Sarnachiaro GO, Sarnachiaro E, Gotta SL, Saito H. Flapless Postextraction Socket Implant Placement in the Esthetic Zone: Part 1. The Effect of Bone Grafting and/or Provisional Restoration on Facial-Palatal Ridge Dimensional Change—A Retrospective Cohort Study. Int J Periodontics Restorative Dent 2014;34:323–331.
27. Trimpou G, Weigl P, Krebs M, Parvini P, Nentwig GH. Rationale for esthetic tissue preservation of a fresh extraction socket by an implant treatment concept simulating a tooth. Dent Traumatol. 2010 Feb;26(1):105-111.
28. Lang NP, Pun L, Lau KY, Li KY, Wong MC. A systematic review on survival and success rates of implants placed immediately into fresh extraction sockets after at least 1 year. Clin Oral Implants Res. 2012 Feb;23 Suppl 5:39-66.
29. Kan JY, Roe P, Rungcharassaeng K, Patel RD, Waki T, Lozada JL, Zimmerman G. Classification of sagittal root position in relation to the anterior maxillary osseous housing for immediate implant placement: a cone beam computed tomography study. Int J Oral Maxillofac Implants. 2011 Jul-Aug;26(4):873-876.
30. Kan JY, Rungcharassaeng K, Umezu K, Kois JC. Dimensions of peri-implant mucosa: an evaluation of maxillary anterior single implants in humans. J Periodontol. 2003 Apr;74(4):557-562.
31. Chen ST, Buser D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla–a systematic review. Int J Oral Maxillofac Implants. 2014;29 Suppl:186-215.
32. Kan JY, Rungcharassaeng K, Morimoto T, Lozada J. Facial gingival tissue stability after connective tissue graft with single immediate tooth replacement in the esthetic zone: consecutive case report. J Oral Maxillofac Surg. 2009 Nov;67(11 Suppl):40-48.
33. Yoshino S, Kan JY, Rungcharassaeng K, Roe P, Lozada JL. Effects of connective tissue grafting on the facial gingival level following single immediate implant placement and provisionalization in the esthetic zone: a 1-year randomized controlled prospective study. Int J Oral Maxillofac Implants. 2014 Mar-Apr;29(2):432-440.
34. Buser D, Chen ST, Weber HP, Belser UC. Early implant placement following single-tooth extraction in the esthetic zone: biologic rationale and surgical procedures. Int J Periodontics Restorative Dent. 2008 Oct;28(5):441-451.
35. Buser D, Chappuis V, Kuchler U, Bornstein MM, Wittneben JG, Buser R, Cavusoglu Y, Belser UC. Long-term stability of early implant placement with contour augmentation. J Dent Res. 2013 Dec;92(12 Suppl):176S-82S.
26. Sanz I, Garcia-Gargallo M, Herrara D, Martin C, Figuero E, Sanz M. Surgical protocols for early implant placement in post-extraction sockets: a systematic review. Clin Oral Implants Res. 2012 Feb;23 Suppl 5:67-79.
37. Schropp L, Isidor F. Timing of implant placement relative to tooth extraction. J Oral Rehabil. 2008 Jan;35 Suppl 1:33-43.











