
Introduction
Congenital granular cell epulis (CE) is a rare benign tumor occurring exclusively in neonates. The term “epulis” derives from the Greek word meaning “on the gingiva”.1 It was first described by Neumann in 1871, and is sometimes referred to as Neumann’s tumor or congenital epulis of the newborn.1 Approximately 200 cases have been documented to date.2 The lesion clinically appears as a sessile or pedunculated, non-ulcerated, smooth, pink to reddish mass. The most common location is the maxillary alveolar ridge at the future location of the maxillary canine. The CE presents eight to 10 times more frequently in females and three times more frequently in the maxilla than in the mandible.2 It is typically a solitary entity; however, multiple lesions in the same or different alveolar ridges have also been reported.3 Histologically, the lesion shows characteristic large polyhedral cells with abundant granular cytoplasm and small nuclei.
Histogenesis is uncertain, though several theories of origins have been postulated, namely odontogenic, fibroblastic, histiocytic, myoblastic and neurogenic.4 The lesion shows benign behavior and tendency of recurrence or malignant transformation has not been reported to date. The purpose of this report is to present and discuss management of a typical case of congenital epulis of a four-day-old newborn causing feeding problems.
Case Report
A four-day-old girl was referred to the emergency department at British Columbia Children’s Hospital for examination of a mass protruding from her mouth. The infant’s pediatrician referred her for an assessment as an outpatient; however, her mother was concerned as the infant was experiencing difficulty with breastfeeding. The mass was noticed at birth but was reported to have changed from a pink-red appearance to blue-purple within the last 24 hours. The infant is the firstborn to a Caucasian female and Asian male. The pregnancy was normal and vaginal delivery occurred at 41 weeks. Apgar scores were normal at nine after one minute, and nine after five minutes. The infant weighed 3343 grams at birth. No family history of hereditary diseases was reported.
On clinical examination, a pedunculated, firm, smooth, blue-purple, approximately 1 cm in diameter round, soft tissue mass was found to be attached to the anterior gingiva of the left maxilla by a very thin pedicle. The mass prevented normal closure of the mouth but posed no immediate airway concerns. The infant’s weight was 3142 grams, decreased by six percent since birth. General physical examination was otherwise normal.
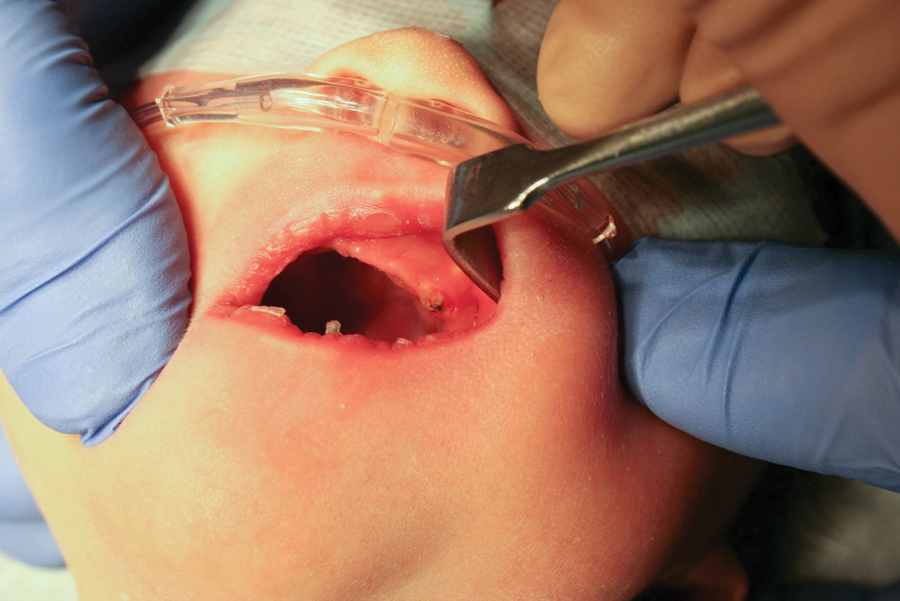
Due to the patient’s decreasing weight, potential airway complication and parental apprehension, she was taken to the operating room on the same day as her initial examination. An excisional biopsy was performed using electrocautery under general anesthesia (Fig. 1). The specimen, measuring 1.0cm x 1.0cm x 0.8cm (Fig. 2), was submitted to the pathology laboratory for histological analysis. There was minimal intraoperative hemorrhage and hemostasis was achieved without any sutures (Fig. 3). Oral feedings were instituted on the first postoperative day and the infant was discharged the same day. One-week after surgery, the patient was seen and noted to be thriving and gaining weight.
FIGURE 1. Preoperative appearance of a large pedunculated intraoral mass arising from the gingiva of the left anterior maxilla in a four-day-old neonate female.

FIGURE 2. Excised pedunculated lesion measuring 1 cm x 1 cm x 0.8 cm.

FIGURE 3. Postoperative appearance of the electrocauterized site.
Histological examination of the specimen revealed characteristic large polyhedral cells with abundant granular eosinophilic cytoplasm and small round nuclei (Fig. 4). The specimen was negative for S-100 protein staining, and positive for CD-68 staining (Fig. 5). These findings are consistent with the diagnosis of CE.
FIGURE 4. Section through the tumor stained with hematoxylin and eosin, high-power microscopy showing characteristic polygonal cells with granular cytoplasm and small nuclei.

FIGURE 5. Immunostaining with CD-68 showing positive cytoplasmic hyaline globules.

Discussion
This case describes a classical presentation of CE found in a healthy four-day-old newborn. The presence of a pedunculated, smooth, round and firm mass in the left anterior maxillary alveolar ridge prevented the infant from latching onto the breast. The CE is usually pink to reddish in color. The reported history of color change to blue-purple could be the result of torsion of the pedunculated mass around its thin stalk that altered the lesion’s vascular supply. There have been nine reports in the literature that documented spontaneous regression of lesions as large as 1.5 cm in diameter.5 However, when the lesion is causing feeding difficulty or airway concern, the recommended treatment is complete surgical excision under local or general anesthesia. Electrocautery was used in this case and provided excellent hemostasis with minimal intraoperative bleeding. Other reports have shown good outcomes using carbon dioxide and erbium, chromium: yttrium-scandium-gallium-garnet (Er, Cr: YSGG) lasers for CE removal.6,7 CE has not shown to recur after surgical excision, even when the removal has been incomplete. 8 A conservative surgical approach is generally favorable. Future dentition was not found to be affected – except in one case that reported hypoplasia of the primary maxillary left incisor, canine, and first molar in the region where a large 2.5cm CE was surgically removed 11 days after birth.9
The etiology of CE remains a controversy. Histologically, it is similar in appearance to the granular cell tumor and features large polygonal cells with abundant eosinophilic cytoplasm and small nuclei.6 In contrast to the granular cell tumor, a neoplastic lesion of neural origin, CE typically does not stain for S-100 protein, although weak immunopositivity has also been reported in literature.10 In our case, the specimen was positive for the macrophage marker CD-68, supporting a mesenchymal origin.6
CE is generally an isolated finding and it is not associated with any other medical condition or syndrome. However, previous reports have shown its occurrence in infants with polydactyly, goiter, Triple X syndrome, polyhydramnios, maxillary hypoplasia and neurofibromatosis.5
In this case, the lesion was not detected by routine pre-natal ultrasounds. However, the use of 3D ultrasound has enabled further assessment of fetal swallowing and airway patency. There are reports of antenatal diagnoses of CE in fetuses as early as 31 weeks in gestation.11 Ex utero intra-partum treatment for an obstructive lesion diagnosed in the fetus in the pre-natal period has been reported and involved an interdisciplinary team.12 It is speculated that the CE exhibits maximal growth under hormonal influences later in gestation, at the end of the third trimester.13
On examination of an intraoral mass in the neonate, the clinician should also consider differential diagnoses of congenital malformations such as encephalocoele, dermoid cysts or teratoma and benign and malignant neoplasms including hemangioma, lymphatic malformations and rhabdomyosarcoma.14 OH
Acknowledgement:
The authors wish to thank Dr. Jason Choi, a staff oral and maxillofacial surgeon, BC Children’s Hospital, for his expertise in the surgical management of this case.
Dr. Sun is a staff pediatric dentist at British Columbia Children’s Hospital and a clinical assistant professor, Faculty of Dentistry, University of British Columbia, Vancouver, British Columbia, Canada.
Dr. Cheung is a staff pediatric dentist at British Columbia Children’s Hospital and a clinical associate professor, Faculty of Dentistry, University of British Columbia, Vancouver, British Columbia, Canada.
Oral Health welcomes this original article. Remaining references can be viewed on our website at www.oralhealthgroup.com.
References:
1. Neumann E. Ein von congenital epulis. Arch Heilkd 1871;12:189-90.
2. Bang KO, Bodhade AS, Dive AM. Congenital granular cell epulis of a newborn. Dent Res J 2012;9:S136-8.
3.Childers EL, Fanburg-Smith JC. Congenital epulis of the newborn: 10 new cases of a rare oral tumor. Ann Diagn Pathol 2011;15:157-61.
4. Merrett SJ, Crawford PJ. Congenital epulis of the newborn: a case report. Int J Paediatr Dent 2003;13:127-9.
5. Ritwik P, Brannon RB, Musselman RJ. Spontaneous regression of congenital epulis: a case report and review of the literature. J Med Case Rep 2010; 21:331-4.
6. Lapid O, Shaco-Levy R, Krieger Y, Kachko L, Sagi A. Congenital epulis. Pediatrics 2001 Feb;107(2):E22.
7. Olivi G, Constacurta M, Maturo P, Cocinmo R: Removal of a fibrous epulis with Er, Cr: YSGG laser: case report. Eur J Paediatri Dent 2007;8:149-52.
8. Anderson PJ, Kirkland P, Schafler K, Moss AL. Congenital gingival granular cell tumour. J R Soc Med 1996; 89(1):53-4.
9. Sunderland R, Sunderland EP, Smith CJ: Hypoplasia following congenital epulis. Br Dent J 1984;157:353.
10. Adeyemi BF, Oluwasola AO, Adisa AO. Congenital epulis. Indian J Dent Res 2010 Apr-Jun;21(2):292-4.
11. Kusukawa J, Kuhara S, Koga C, Inoue T. Congenital granular cell tumor (congenital epulis) in the fetus: a case report. J Oral Maxillofac Surg 1997 Nov;55(11):1356-9. Erratum in: J Oral Maxillofac Surg 1998;56:694.
12. Kumar P, Kim HH, Zahtz GD, Valderrama E, Steele AM: Obstructive congenital epulis: prenatal diagnosis and perinatal management. Laryngoscope 2002;112:1935-9.
13. Kim SK, Won HS, Lee SW, et al. Prenatal diagnosis of congenital epulis by three-dimensional ultrasound and magnetic resonance imaging. Prenat Diagn 2006;26:171-4.
14. McGuire TP, Gomes PP, Freilich MM, Sándor GK. Congenital epulis: a surprise in the neonate. J Can Dent Assoc 2006;72:747-50.











