

Following orthodontic treatment, retention is fundamental in maintaining teeth in their corrected positions. Irrespective of the patient’s age, underlying malocclusion, or type of mechanotherapy used, retention is necessary to preserve the final alignment and occlusion. Without retention, there is a natural tendency for teeth to relapse back towards the original malocclusion. This article will highlight the different types of removable and fixed retainers, including their indications, advantages, limitations, duration of wear, and proper management.
GOALS OF RETENTION
The main goals of the retention phase following orthodontic tooth movement are to:
1) Allow for reorganization of the gingival and periodontal tissues. Forces from the gingival and periodontal fibres around the teeth tend to pull the teeth back towards their original positions.
2) Minimize changes due to growth and aging. In late adolescence, continued growth in the patterns that contributed to the initial malocclusion can affect the stability of the orthodontic outcome. In addition, long-term studies have shown that very slow growth continues throughout adult life.1 These age changes in the form of ongoing dentofacial growth and changes in the surrounding soft tissues can contribute to the deterioration of occlusal relationships and tooth alignment.
3) Maintain teeth in unstable positions. The teeth may be in an inherently unstable position after treatment sometimes necessary due to compromise or aesthetics.
4) Permit neuromuscular adaptation to the corrected tooth position. Continuous soft tissue pressures may more readily produce a relapse tendency.
Due to the variable number of factors at play that can lead to relapse or unwanted tooth movement, it is essential that orthodontists, patients and their primary dental practitioners (PDP) understand the importance of wearing retainers after orthodontic treatment.
TYPES OF RETAINERS
A Cochrane Review carried out to evaluate the effects of different methods of retention reported that there was insufficient high-quality evidence on the best type of retainer or retention regimen.2 With that, each practitioner’s approach to retention will be greatly influenced by their clinical experience and expertise with different retainers in addition to the patient’s preferences, expectations and circumstances.
Retainers can be broadly classified as either fixed or removable.
Removable retainers can be removed by the patient, which affords the advantage of being easier to fully clean around the teeth to maintain proper oral hygiene. Part-time or full-time wear may be prescribed; however, it has been shown that in many cases, removable retainers need only be worn at night to maintain dental stability.3,4,5 Excellent compliance is essential with removable retainers, and if consistent wear is overlooked, relapse can occur.
Fixed retainers are bonded to the teeth and are in place permanently which reduces the demands on patient compliance. However, as they cannot be removed for cleaning, they are more prone to plaque and calculus accumulation and may hinder a patient’s oral care practices.6
The main types of retainers are discussed in Tables 1, 2, and 3.
Table 1: Removable Essix (Vacuum-Formed) Retainers
Materials and Design:
- Fabricated by softening a clear thermoplastic polymer sheet through heat and then moulding it over working models of the teeth by either vacuum or pressure thermoforming.
- The thin and transparent design makes them a discreet retainer option that is well accepted by patients from a comfort and aesthetic perspective.
- Currently the most widely used retainer for the maxillary arch.7


Advantages:
- Ease of fabrication and can be made quickly on the same day as appliance removal.
- Relatively inexpensive.
- Patient comfort and acceptability.
- Can be modified to produce minor active tooth movements if required.
- Prosthetic teeth can be incorporated in cases with hypodontia.
Limitations:
- Restorations or changes to the anatomy of teeth may alter the fit and necessitate fabrication of a new retainer.
- Due to the lack of palatal coverage, they are not able to control deepening of the bite.
- Occlusal coverage of the most distal molars is essential, otherwise there is risk of over-eruption of these teeth.8
- Tend to crack and discolour over time.
- Patients should not eat or drink with the retainers in place as this can lead to higher risk of caries.
- Due to their inherent flexibility, they cannot be used to retain cases where palatal expansion was achieved.
- Not suitable for patients who are in mixed dentition where further tooth eruption is anticipated.
- The thickness of material over the occlusal surface of the teeth can be problematic if both arches are retained in this way due to the intrusive forces on the posterior teeth.
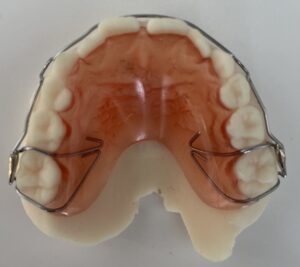
Table 2: Removable Acryclic Retainers (Hawley And Begg Type Retainers)
Materials and Design:
- Constructed from a wire framework and acrylic baseplate.
- The retentive wire components are custom-made usually from a 0.7-0.9 mm stainless steel wire.

Advantages:
- Robust and can last for many years.
- Can be worn when eating without becoming damaged.
- Is able to facilitate posterior occlusal settling during retention.9
- Can be modified for simple active tooth movements if required by activating the labial bow or by incorporating springs.
- Due to the palatal coverage, it inherently provides a potential bite plane to control overbite and an anterior bite plane can be incorporated to further help retain corrected deep overbites.
- Prosthetic teeth can be added and designed to act as space maintainers to prevent any movement of future abutment teeth.
Limitations:
- Speech difficulties in the initial period of wear.
- Poor esthetics due to the visible metal labial bow.
- Can result in embarrassment or lack of confidence (due to speech issues and high visibility of the appliance) which may negatively affect compliance with wear.
- Does not reliably keep premolar extraction spaces closed especially in designs where the labial bow crosses the extraction site.
Table 3: Fixed Bonded Retainers
Materials and Design:
- There are multiple designs with a fixed retainer: the wire material can be a smooth wire, metal chain, or multi-strand wire that is bonded to all six anterior teeth or just the canines.
- Can be bonded with a direct or indirect technique where the retainer is attached to the lingual surface of the teeth and bonded in position using a light-cured composite resin.
Indications:
- Following orthodontic closure of a spaced dentition (including large diastemas).
- After the creation of anterior space prior to prosthodontic management.
- In cases where there is reduced periodontal support.
- Following correction of severe rotations.
- After significant labial-lingual changes in tooth position have occurred.
- In compromised cases where improved alignment and aesthetics have been achieved; however, a non-ideal occlusion has been accepted.


Advantages:
- Can increase periodontal ligament stability and can act as a splint in cases where there is compromised periodontal support.
- Discreet.
- In place permanently which removes the need for patient compliance with retainer wear.
- Robust and can last for many years.
- Can be worn when eating without becoming damaged.
Limitations:
- Possible hygiene difficulties.
- Risk of localized relapse where there is a partial debond of the retainer.
- Risk of decalcification and caries in undetected debonds.
- More prone to plaque and calculus accumulation as they cannot be removed for cleaning.10
- Faulty or incorrectly repaired retainers may become active and cause unwanted tooth movement.
- When placing maxillary bonded retainers, care should be taken to clear the occlusion and minimize occlusal contacts with the opposing lower teeth as these contacts have shown to increase failure rates. – Therefore, they may not be suitable in some deep bite cases.
DURATION OF RETENTION
Subtle facial growth continues to occur throughout life. This manifests as both skeletal changes in the maxilla and mandible and also changes to the surrounding soft tissue and their pressures exerted on the dentition.11 Therefore, it is not surprising that there is always the potential for changes to occur in the alignment of teeth and occlusal relationships with time due to the fact that the dentition exists within a dynamic biological environment that is constantly changing. Consequently, it is advocated that indefinite retention should be used following orthodontic tooth movement to minimize both relapse and maturational changes. Orthodontic retention is a life-long commitment.
THE PDP’S ROLE IN ORTHODONTIC RETENTION
Properly managing a patient’s retention protocol will minimize any unwanted effects on oral health and orthodontic outcomes. It should be emphasized that the PDP can play a key role in supporting patients with their retention regime. This can include informing current and potential orthodontic patients that wearing retainers after treatment is an essential part of orthodontic treatment, reinforcing the need for patients to wear their retainers, motivating patients to adhere to their retention protocol, checking that bonded retainers are still intact, ensuring that good oral hygiene is being maintained around patients’ retainers, monitoring when retainer repair or replacement is needed, and liaising with the orthodontist as required.12
CONCLUSION
Retention is necessary following orthodontic tooth movement. Relapse after orthodontic treatment is the result of teeth moving back towards the original malocclusion, but also due to changes in tooth position that may occur as part of the normal growth and aging process. Due to the unpredictable nature of relapse, it is advocated that indefinite retention is used following tooth movement. Since there is currently insufficient research data on which to base clinical practice on retention, each clinician should have a good understanding of the different types of retainers along with their indications, advantages, and limitations.
Oral Health welcomes this original article.
References
- Behrents RG. A treatise on the continuum growth in the aging craniofacial skeleton. Ann Arbor, Mich: University of Michigan Center for Human Growth and Development; 1984.
- Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Worthington HV. Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database of Systematic Reviews 2016, Issue 1. Art. No.: CD002283.
- Gill DS, Naini FB, Jones A, Tredwin CJ. Part-time versus full-time retainer wear following fixed appliance therapy: a randomized prospective controlled trial. World Journal of Orthodontics 2007;8:300–306.
- Shawesh M, Bhatti B, Usmani T, Mandall N. Hawley retainers full or part time? A randomized clinical trial. Eur J Orthod 2010;32:165–170.
- Thickett E, Power S. A randomized clinical trial of thermoplastic retainer wear. Eur J Orthod 2010;32:1–5.
- Millett DT, McDermott P, Field D, et al. Dental and Periodontal Health with Bonded or Vacuum-formed Retainer. In: IADR Conference Abstract 3168. Toronto, 2008
- Proffit, William R. Contemporary Orthodontics / William R. Proffit … [et Al.]. 5th ed. St. Louis, Mo: Elsevier/Mosby, 2013. Print.
- Chate R A, Falconer D T. Dental appliances with inadequate occlusal coverage: a case report. Br Dent J 2011; 210: 109–110.
- Sauget E, Covell D A, Boero R P, Lieber W S. Comparison of occlusal contacts with use of Hawley and clear overlay retainers. Angle Orthod 1997; 67: 223–230.
- Littlewood SJ, Kandasamy S, Huang G. Retention and relapse in clinical practice. Aust Dent J. 2017 Mar;62 Suppl 1:51-57.
- Behrents RG, Harris EF, Vaden JL, Williams RA, Kemp DH. Relapse of orthodontic treatment results: growth as an etiological factor. J Charles H Tweed Int Found 1989;17:65–80.
- Johnston CD, Littlewood SJ. Retention in orthodontics. Br Dent J. 2015 Feb 16;218(3):119-22.
About the Author:

Dr. Vanessa Chong is an orthodontist in private practice in Toronto, Ontario. She is board-certified in Orthodontics in both Canada and the USA.








