

Despite the recent growth of clear aligner therapy, fixed appliances–i.e., braces–are still the most used orthodontic appliance worldwide. The large majority of braces systems currently on the market are “one size fits all” pre-fabricated brackets that apply the same generic prescription to every patient, despite significant individual differences in malocclusion type and tooth anatomy. Achieving an ideal result with these conventional appliance systems often requires time consuming wire bending and bracket repositioning1. Another challenge is that bonding of conventional braces is typically done manually and is prone to positioning errors2. These factors diminish the efficacy and efficiency of traditional braces treatment, and it has become apparent that a new solution for braces is needed for the digital age.
What is LightForce?
LightForce Orthodontics was founded in 2015 to create a personalized braces system utilizing 3D printing. (Fig. 1) 3D printing is well suited for orthodontics, at is excels at creating small, complex parts at scale. In addition, the digital milieu of 3D printing enables innovation in hardware (brackets) at the speed of software development, allowing rapid innovation and product evolution. LightForce received FDA approval in 2019 and has revolutionized fixed appliance therapy by providing orthodontists with a digital, clinically effective, and fully customized braces system.
Fig. 1A

Fig. 1B

LightForce Digital Workflow
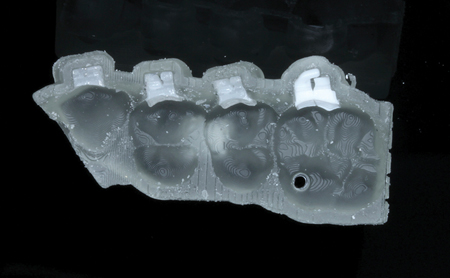
Initiating treatment with LightForce requires submission of a prescription form and digital diagnostic records including an intra-oral scan, radiographs, and photographs. A LightPlan (cloud-based proprietary case planning software) is then created to achieve an ideal set-up of the dentition based on the treatment goals. Customized brackets are digitally designed by the software to achieve the patient-specific tooth positions. (Fig. 2) Once the doctor edits and approves the case set-up, polycrystalline alumina (ceramic) brackets are 3D printed in LightForce’s advanced manufacturing facility, placed in 3D printed indirect bonding trays (Fig. 3) and shipped to the orthodontic practice for indirect bonding.
Fig. 2
Fig. 3
How are LightForce Brackets Unique?
Unlike conventional brackets, which are generically fabricated by the thousands with standard manufacturing techniques (e.g., injection molding), LightForce brackets are designed de novo for each tooth. (Fig. 4) The anatomically customized bracket base, individualized prescription, and dimensionally accurate wire slot (Fig. 5A) enable the orthodontist to achieve precise tooth movement in all dimensions without significant wire bending or bracket repositioning.
Fig. 4A

Fig. 4B

Fig. 5A

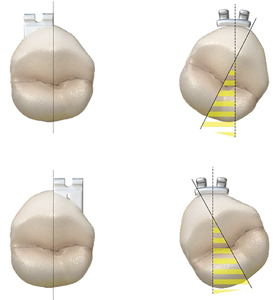
A unique feature of LightForce brackets is that they do not need to be centered horizontally on the facial axis of the teeth, as the custom base can compensate for any potential rotations. (Fig 5B) Additional features of LightForce brackets are customizable hooks, digitally designed and indirectly bonded bite turbos, a choice of wire slot sizes, a choice of two esthetic bracket colors (white or translucent), and the inclusion of an extra set of brackets in single tooth indirect bonding trays for easy bracket replacement during treatment.
Fig. 5B
Clinical Advantages of using LightForce
Retrospective data3 has demonstrated that treatment with LightForce may reduce the total treatment time and number of appointments compared to conventional braces. LightForce was also shown to improve the quality of the treatment result as measured by the Peer Assessment Rating (PAR) Index4,5. Relative to removable clear aligners, LightForce braces require less patient compliance and can be used in a wide range of case type and complexity.
Case Reports
The following case reports highlight the efficacy of LightForce braces. Some cases were treated prior to the availability of custom molar tubes, which are currently available on first and second molars.
Case I
A 12-year-old female presented with a general concern regarding the appearance of her teeth. (Fig. 6) Upon examination, we noted a Class II malocclusion with excessive overjet, negative crown torque in the maxillary bicuspids, and a maxillary transverse excess relative to the lower arch. Treatment planning benefited from a custom prescription to add positive torque (buccal crown inclination) to the maxillary bicuspids to enhance the posterior smile display and to upright the lower posterior teeth to create a better occlusion. These movements were programmed with LightForce software but would have been difficult to achieve with a conventional appliance, as negative torque in the posterior segments is an inherent part of all standard braces prescriptions and may have prevented the achievement of the esthetic and occlusal goals. Accurate bracket placement was enabled by LightForce’s advanced indirect bonding system. (Fig 7) An excellent esthetic and functional result was obtained, (Fig. 8) and the treatment was completed with Nickel Titanium wires and no wire bending.
Fig. 6A

Fig. 6B

Fig. 6C

Fig. 6D

Fig. 7A

Fig. 7B

Fig. 8A

Fig. 8B

Fig. 8C

Fig. 8D

Case II
A 14-year-old female presented with a congenitally missing lower incisor, a large maxillary midline diastema, and a gingival smile. (Fig 9A) It was important to preserve her smile arc6 and this was achieved with careful digital planning in LightPlan to avoid over-intrusion of the maxillary incisors. (Fig 9B) The excessive gingival smile was corrected with gingivectomies. Custom planning of anterior torque values helped solve the Bolton discrepancy caused by the missing incisor. The accuracy of LightForce’s indirect bonding system (Fig 10) and the clinical performance of the custom brackets contributed to an ideal result (Fig 11) without wire bending.
Fig. 9A

Fig. 9B

Fig. 9C

Fig. 9D

Fig. 9E

Fig. 9F

Fig. 10

Fig. 11A

Fig. 11B

Fig. 11C

Fig. 11D

Fig. 11E

Case III
A 28-year-old female presented with a skeletal class III malocclusion characterized by posterior cross-bite, anterior open-bite, anterior edge-to-edge occlusion, significant crowding, occlusal plane cant in both arches, and gingival recession. (Fig 12) The treatment plan involved combined orthodontic treatment with orthognathic surgery. Digital planning (Fig 13) and accurate indirect bonding enabled precise pre-surgical occlusal preparation. The oral and maxillofacial surgeon was pleased with the well interdigitated pre-surgical models and was able to achieve an ideal surgical outcome. (Fig 14) Final records show improved alignment, occlusion, and smile esthetics, and highlight the benefits of utilizing LightForce braces for patients requiring orthognathic surgery or other complex treatments. (Fig 15)
Fig. 12A

Fig. 12B

Fig. 12C

Fig. 12D

Fig. 12E

Fig. 13

Fig. 14A

Fig. 14B

Fig. 15A

Fig. 15B

Fig. 15C

Fig. 15D

Fig. 15E

Fig. 15F

Conclusion
LightForce fully individualized 3D printed braces represent a turning point in the history of fixed orthodontic appliances. Equipped with this novel clinical tool, orthodontists now have the ability to apply their knowledge of biology, occlusion, and esthetics in new and creative ways to achieve customized results for their patients.
Oral Health welcomes this original article.
Disclosures: Dr. Alexander Waldman is a Clinical Executive Board Member and Shareholder for LightForce.
References
- Creekmore TD, Kunik RL. Straight wire: The next generation. Am J Orthod Dentofacial Orthop. 1993;104(1):8-20.
- Koo BC, Chung CH, Vanarsdall RL. Comparison of the accuracy of bracket placement between direct and indirect bonding techniques. Am J Orthod Dentofacial Orthop. 1999;116(3):346-351. doi:10.1016/S0889-5406(99)70248-9.
- Waldman A, Garvan CS, Yang J, Wheeler TT. Clinical efficiency of LightForce 3D-printed custom brackets. J Clin Orthod JCO. 2023;57(5):274-282.
- Green JI. An Overview of the Peer Assessment Rating (Par) Index for Primary Dental Care Practitioners. Prim Dent J. 2016;5(4):28-37. doi:10.1308/205016816820209460.
- Richmond S, Shaw WC, O’Brien KD, et al. The development of the PAR Index (Peer Assessment Rating): reliability and validity. Eur J Orthod. 1992;14(2):125-139. doi:10.1093/ejo/14.2.125.
- Sarver DM. The importance of incisor positioning in the esthetic smile: The smile arc. Am J Orthod Dentofacial Orthop. 2001;120(2):98-111. doi:10.1067/mod.2001.114301.
About the Author

Dr. Alexander Waldman is a board-certified orthodontist passionate about helping patients of all ages achieve a beautiful smile and healthy bite. Dr. Waldman received his undergraduate and dental degrees from the University of Pennsylvania and completed his clinical orthodontic training and Master of Medical Science at Harvard University. Dr. Waldman founded Waldman Orthodontics in Beverly Hills, CA, combining the latest digital advancements in orthodontics with evidenced-based practice. In addition to his clinical experience, Dr. Waldman is an educator, author, and advisor to multiple start-ups in the orthodontic and dental industries.








