
The common answer is ‘It depends on the manufacturer’s instructions’. The resin manufacturer or the light manufacturer? What if they do not agree? Many aspects of restorative dentistry are based upon clinical learning or creativity. However, composite curing is not one of them. Hence, “how long to cure my composite” is a common dilemma.
There is no universal length of time that will cure all resins. A specified amount of light (energy) must be delivered to cure the composite resin.1 (How long to fill a bucket with water is a good analogy – it depends on the size of the bucket and the water flow rate.)
Some terminology
Joule – energy unit transferred to an object. For a dental curing light, this is the electrical energy transferred to the LEDs to produce light energy which excites photoinitiators in the composite to produce chemical energy that, in turn, links resin monomers. Energy (measured in Joules) is a measure of power (measured in Watts) multiplied by time.2 Thus, a curing light must deliver an adequate power for a sufficient amount of time to produce the required amount of energy to the resin-based composite.
Irradiance (mW/cm2) – power (in mWatts) of the light divided by the surface area (cm2) of the light tip. When calculating the required curing energy, irradiance is multiplied by the exposure time. Once the manufacturer has determined the necessary curing energy, and given the irradiance of the curing light, the required exposure time can be calculated. (If ten Joules/cm2 is the polymerization requirement, and the light provides 1000 mW/cm2, then ten seconds of cure are required, and this information is listed in the manufacturer’s instructions for use or IFU.)
This formula implies that increasing the power of the light can be used to decrease the exposure time. Unfortunately, the Exposure Reciprocity Law does not always work. One can measure the efficiency at which light energy delivered to composite is converted to chemical energy within the material by calculating the free radicals formed by the photoinitiators. In comparing, six J/cm2 delivered at 150 mW/cm2 for 40 seconds to 600 mW/cm2 for ten seconds, the longer exposure produced more free radicals.3,4
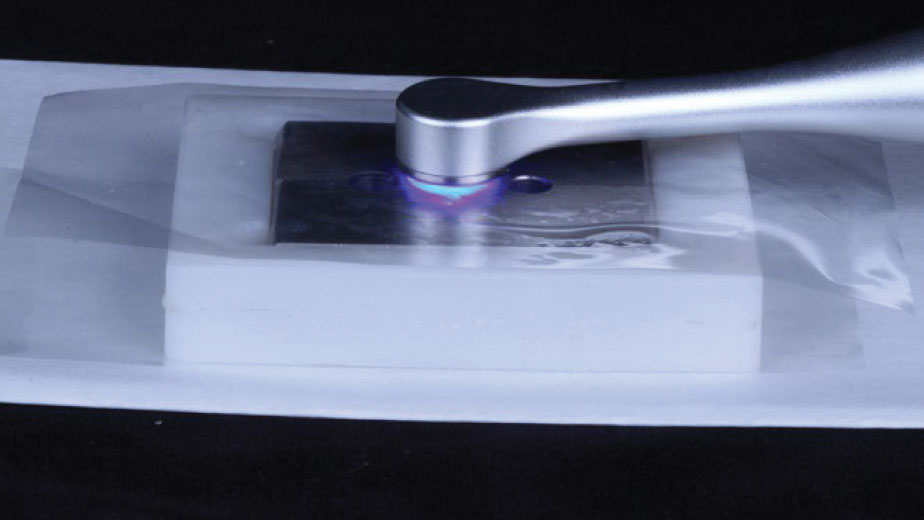
Depth of cure is an easier means for determining the efficiency of light energy conversion into chemical energy. The depth of cure is measured by placing the composite into a cylindrical metal mold (Fig. 1) and then curing it only from the top (Fig. 2). The mold is disassembled, and the uncured composite at the bottom is scraped away (Fig. 3). The depth of the remaining cured composite is measured, and halved to determine the depth of cure (Fig. 5). The composite in the bottom half has not completely polymerized to full physical maturity and bond strength (Fig. 4).5
Fig. 1
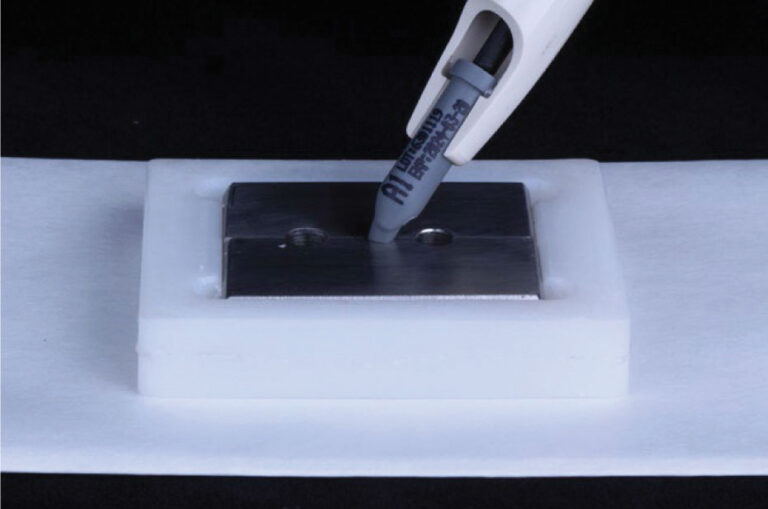
Fig. 2

Fig. 3
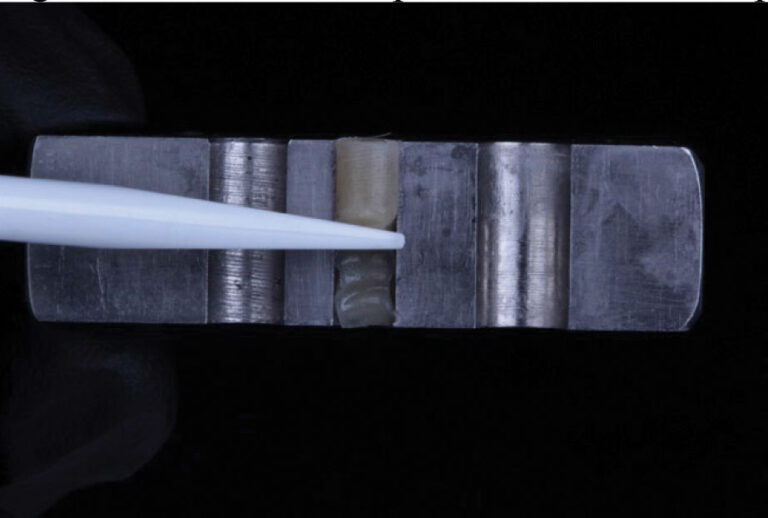
Fig. 4
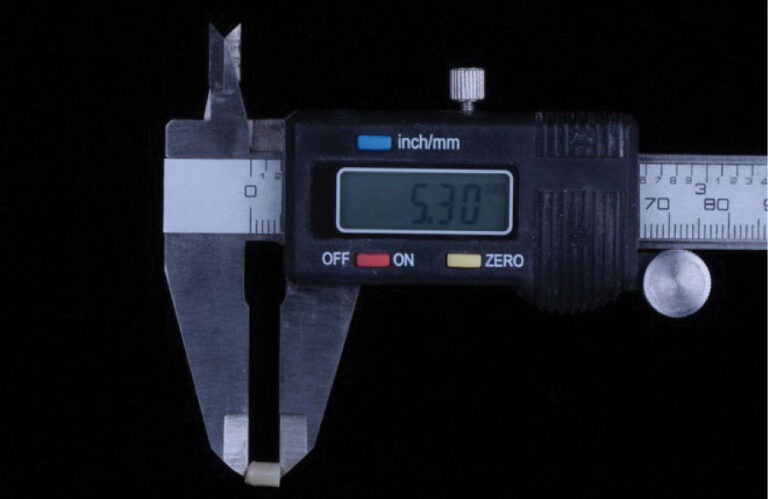
Fig. 5

It is most beneficial to compare polymerization depths with the same curing light and composite. The WOLFLlight Cure-FX curing light (Dental Savings Club, Montreal QC) and Phil Nano composite (Dental Savings Club, Montreal QC) were utilized. The WOLFLlight Cure-FX curing light delivers two levels of irradiance: 1200 mW/cm2 and 2000 mW/cm2. At 1200 mW/cm2 for ten seconds, the depth of cure was 2.4mm. At 2000 mW/cm2 for three seconds, the depth of cure was 2.0mm. These results show that a shorter cure time, at a higher irradiance, achieves a predictable 2mm depth of cure for this composite.
Some practitioners have expressed concern that delivering light energy too quickly speeds polymerization, increasing shrinkage stress. Enroute to vitrification (full-cure), monomers may momentarily exist in a gel-phase wherein de-stressing rearranging movement may occur, decreasing polymerization shrinkage at the bonded interfaces. Alternatively, slower polymerization of the resin may increase polymer length while decreasing cross-linking. This reduces the stiffness/flexibility of the composite resin after vitrification, placing less stress on the bonded interface.6
Various destressing strategies include ramping (slowly increasing irradiance during polymerization), pulse-delay curing (brief intermediate irradiance followed by a waiting period and then followed by high irradiance), and two-step curing (low initial irradiance followed by high irradiance). These approaches attempt to prolong the gel-stage, allowing more monomer rearrangement prior to vitrification.6 A recent theory postulates that pulse-delay curing decreases shrinkage stress by initiating polymerization without vitrification, allowing a cooling of the composite immediately before complete curing with the second-step high irradiance.7
Manufacturers test the depth of composite cure within the diameter of the light tip, at the center, at 0 mm distance. It is essential to remember that only the composite directly under the curing light tip receives the required amount of energy to adequately cure in the manufacturer’s recommended exposure time.8 Curing lights with small tips can only polymerize small composite restorations. Larger restorations require overlapping curing steps, increasing the chairside light curing time. Curing lights with larger tip diameters, such as the WOLF Light’s 9.5mm diameter tip (Fig. 5), are more time-efficient when curing composite resin restorations, particularly in molar teeth.
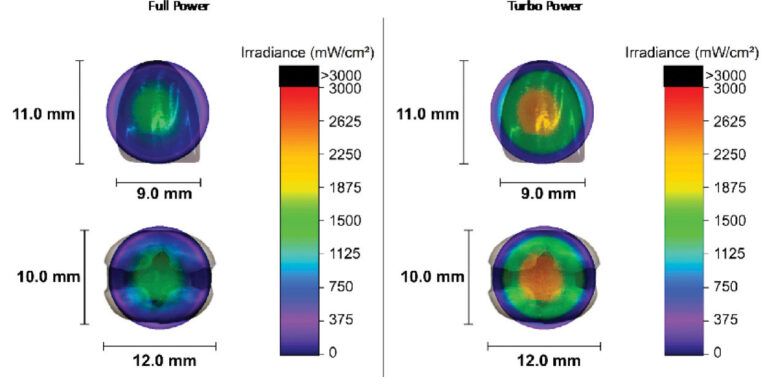
Surface area is not the only criterion, however. Many curing lights have “hot spots” of high irradiance across the tip of the light that cure effectively.9 Unfortunately, their “cold spots” do not polymerize well. Beam profiling is used to map the output across the tip of dental curing lights. A beam profile that has high irradiance at the center and low irradiance at the periphery effectively decreases the useful surface area of the curing light tip. In contrast, a beam profile that has a more even distribution of light across the face of the curing tip is advantageous in avoiding overlapping curing and increased chairside time. Figure 6 presents the beam profile of the WOLFLlight Cure-FX curing light overlaid on anterior and posterior restorations.
Fig. 6
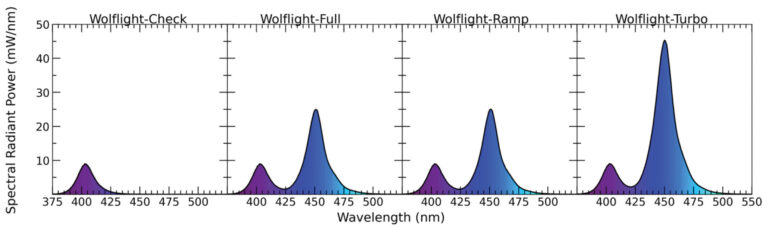
Correct emission wavelength is needed to activate the photoinitiators embedded in the composite. Most composites utilize camphoroquinone with a peak absorbance 468nm. Some composites (certain translucent shades and bulk fills) use alternative photoinitiators that require shorter wavelengths. Polywave lights emit light in both blue and violet wavelengths (Fig. 7).
Fig. 7
Dental resins require a sufficient amount of energy for adequate polymerization to achieve their manufacturer’s specifications. Curing energy is calculated by multiplying power and time, but the relationship is not necessarily linear. There may be advantages to alternative curing protocols, and there are numerous incidental considerations which may affect the process. Each specific combination of curing light, curing power, length of cure, and composite material should be tested for polymerization depth predictability.
Oral Health welcomes this original article.
References
- Rocha MG, Maucoski C, Roulet JF, Price RB. Depth of cure of 10 resin-based composites light-activated using a laser diode, multi-peak, and single-peak light-emitting diode curing lights. J Dent. 2022 Jul;122:104141. doi: 10.1016/j.jdent.2022.104141. Epub 2022 Apr 25. PMID: 35483497.
- Price RB, Ferracane JL, Shortall AC. Light-Curing Units: A Review of What We Need to Know. J Dent Res. 2015 Sep;94(9):1179-86. doi: 10.1177/0022034515594786. Epub 2015 Jul 8. PMID: 26156516.
- Leprince JG, Lamblin G, Devaux J, Dewaele M, Mestdagh M, Palin WM, Gallez B, Leloup G. Irradiation modes’ impact on radical entrapment in photoactive resins. J Dent Res. 2010 Dec;89(12):1494-8. doi: 10.1177/0022034510384624. Epub 2010 Oct 12. PMID: 20940363.
- Selig D, Haenel T, Hausnerová B, Moeginger B, Labrie D, Sullivan B, Price RB. Examining exposure reciprocity in a resin based composite using high irradiance levels and real-time degree of conversion values. Dent Mater. 2015 May;31(5):583-93. doi: 10.1016/j.dental.2015.02.010. Epub 2015 Mar 21. PMID: 25804190.
- ISO 4049:2019 – Polymer-based restorative materials
- Feng L, Suh BI. A mechanism on why slower polymerization of a dental composite produces lower contraction stress. J Biomed Mater Res B Appl Biomater. 2006 Jul;78(1):63-9. doi: 10.1002/jbm.b.30453. PMID: 16470813.
- Palagummi SV, Hong T, Jiang L, Chiang MYM. Thermal shrinkage reveals the feasibility of pulse-delay photocuring technique. Dent Mater. 2021 Dec;37(12):1772-1782. doi: 10.1016/j.dental.2021.09.007. Epub 2021 Oct 2. PMID: 34607708.
- Price RB, Labrie D, Rueggeberg FA, Sullivan B, Kostylev I, Fahey J. Correlation between the beam profile from a curing light and the microhardness of four resins. Dent Mater. 2014 Dec;30(12):1345-57. doi: 10.1016/j.dental.2014.10.001. PMID: 25460008.
- AlShaafi MM, Harlow JE, Price HL, Rueggeberg FA, Labrie D, AlQahtani MQ, Price RB. Emission Characteristics and Effect of Battery Drain in “Budget” Curing Lights. Oper Dent. 2016 Jul-Aug;41(4):397-408. doi: 10.2341/14-281-L. Epub 2015 Dec 11. PMID: 26652017.
About the Authors:

Dr. Nathaniel Lawson is an Associate Professor and Director of the Division of Biomaterials at the UAB School of Dentistry. Additionally, he is the director of a two year Biomaterials residency program. He is passionate about testing new materials and techniques in the laboratory and applying the results to clinical dentistry. His primary research interests are related to the physical and mechanical properties of dental ceramics, composites, cement, and adhesives.

Dr. Krisha Shah is a resident in the Biomaterials program at the UAB School of Dentistry.








